Pfizer/BioNTech C4591001 Trial - Deaths during the trial.
Clarifying a few figures heard here & there; and yes, BNT162b2 subjects died more than Placebo ones during the trial, as far as we can say given the current data.
Introduction
The following breakdown develops how to identify deaths registered during the trial as per the currently available PHMPT documents1. This article has been co-written with biostatistician Christine Cotton’s2, who cross-checked in depth our figures, and whom we can’t thank enough for her time, her dedication, and expertise.
It aims to clarify how many deaths occurred, and after which dose, during the trial (as far as the documented deaths are concerned, and given the little trust we can have in Pfizer/BioNTech data3).
We then briefly elaborate on Pfizer/BioNTech’s obvious lack of tracking of the subjects, reflected by the figures documented, confronted to the expectible ones.
Deaths in the safety population of the trial
Among the “eligible for safety” population (in the ADSL table4, subjects with tag “SAFFL” = “Y”), we find 43 600 subjects, 23 155 in each arm, in phase 2-3, excluding duplicates (12 subjects with tag MULENRFL = “Y”).
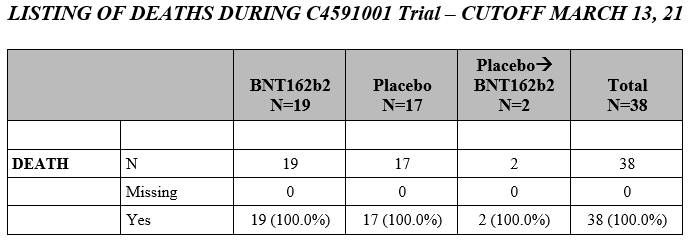
When the files have been exported (their state corresponds in theory to the Biologics Licence Application - BLA5 but some records have been entered afterwards), the “apparent” death of 19 subjects in each treatment arm had been recorded.
A .PDF export, available thanks to PHMPT6, tells us the recorded cause of death of these subjects who died. We detail them below by arm & age group.
We highlight here that the “19 - 19” we often hear is misleading: as we will detail, and the real count is 21 BNT162b2 & 17 Placebo, as synthetized in this table.
Deaths are recorded starting in the age group 35 to 44 years old (yo), with 1 placebo death.
- 11521085, a 42 yo Female, died on 2020-08-26, 8 days after her first dose without documented cause.
The adverse effects documented, accessible in the following Google Spreadsheet, don’t offer more details7.
In the 45 to 54 yo group, 3 deaths were recorded in each group.
In the BNT162b2 arm:
- 10211127, a 54 yo Male, died on 2020-12-19, 88 days after his second dose, of “Cardiac failure congestive”
- 11201266, a 51 yo Male, died on 2021-01-19, 113 days after his second dose, of “Lung cancer metastatic”
- 11271112, a 53 yo Male, died on 2020-12-04, 86 days after his second dose, of “Cardio-respiratory arrest”
In the Placebo arm:
- 10811194, a 51 yo Female, died on 2020-11-04, 37 days after her second dose of “Myocardial infarction”
- 11561124, a 53 yo Male, died on 2020-11-02, 32 days after his second dose of “Overdose”
- 12314987, a 47 yo Male, died on 2020-12-06, 82 days after his second dose of cardio-respiratory arrest.
In the 55 to 64 yo group, 8 deaths were recorded in the BNT162b2 group against 6 deaths in the Placebo group.
In the BNT162b2 arm:
- 10071101, a 56 yo Female, died on 2020-10-21, 63 days after her second dose of “Cardiac arrest”
- 10361140, a 64 yo Male, died on 2021-02-10, 91 days after his second dose of “Road traffic accident”
- 10891073, a 63 yo Female, died on 2020-11-12, 70 days after her second dose of “Chronic obstructive pulmonary disease”
- 11141050, a 63 yo Female, died on 2020-10-19, 42 days after her second dose of “Unevaluable event” (but we know it’s not the vaccine thanks to the relation tag set to “N”)
- 11201050, a 58 yo Female, died on 2020-11-07, 73 days after his second dose, of “Cardiac arrest”
- 11401117, a 58 yo Male, died on 2020-12-29, 117 days after his second dose, of “Cardiac arrest”
- 11561160, a 62 yo Female, died on 2020-12-24, 74 days after her second dose of “Road traffic accident”
- 11621327, a 60 yo Male, died on 2020-09-13, 4 days after his first dose of “Arteriosclerosis” (heart condition caused by the thickening, hardening, and loss of elasticity of the walls of arteries)
In the Placebo arm:
- 10661350, a 58 yo Male, died on 2020-11-03, 16 days after his first dose of “Myocardial infarction”
- 10941112, a 57 yo Female, died on 2020-12-18, 81 days after her second dose of “Acute respiratory failure”
- 11681083, a 64 yo Male, died on 2020-11-18, 65 days after his second dose of “Aortic rupture”
- 12291083, a 55 yo Female (with HIV & chronic respiratory disease), died on 2021-01-05, 76 days after her second dose of “COVID-19 pneumonia”
- 12313972, a 61 yo Female, died on 2020-09-28, 16 days after her second dose of “Haemorrhagic stroke”
- 12315324, a 58 yo Female, died on 2021-01-31, 136 days after her second dose of “multiple organs dysfunction”
In the 65 to 74 yo group, 2 deaths were recorded in the BNT162b2 arm & 6 in the Placebo arm.
In the BNT162b2 arm:
- 11351033, a 67 yo Male originally in the Placebo arm, died on 2021-01-29, 5 days after his third dose (the active product), of non-documented cause.
- 11521497, a 72 yo Male, died on 2020-11-11, 36 days after his first dose of “Shigella sepsis” (infection of the intestines caused by Shigella bacteria)
In the Placebo arm:
- 10191146, a 67 yo Male, died on 2020-12-17, 87 days after his second dose of “Metastases to liver”
- 10271191, a 68 yo Female, died on 2021-02-13, 135 days after her second dose of “Respiratory failure”
- 10841470, a 65 yo Male, died on 2021-01-11, 83 days after his second dose of “Multiple organ dysfunction syndrome”
- 10881126, a 65 yo Male, died on 2020-12-01, Cardiac 70 days after his second dose of “Cardiac arrest”
- 11281009, a 66 yo Male, died on 2020-11-28, 102 days after his second dose of “Pneumonia”
- 12071055, a 65 yo Male, died on 2021-02-09, 76 days after his second dose of “Pneumonia bacterial”
In the 75 to 84 yo group, 7 deaths were recorded in the BNT162b2 arm, against 1 in the Placebo arm.
In the BNT162b2 arm:
- 10391010, a 84 yo Male, died on 2020-11-18, 71 days after his second dose of “Arteriosclerosis”
- 10841266, a 77 yo Male, died on 2021-01-12, 121 days after his second dose of “Sepsis”, with “Congestive heart failure” listed in co-morbidities.
- 10881139, a 82 yo Male, died on 2021-03-06, 143 days after his second dose of “Metastases to lung”
- 11291166, a 78 yo Female, died on 2021-02-03, 129 days after her second dose of “Myocardial infarction”
- 11311204, a 84 yo Male originally in the Placebo arm, died on 2021-02-15, 26 days after his third dose of “Cardio-respiratory arrest”
- 11361102, a 76 yo Male, died on 2020-12-19, 31 days after his second dose of “Cardiac arrest”
- 12521010, a 80 yo Male, died on 2020-12-26, 110 days after his second dose of “COVID-19 pneumonia”
In the Placebo arm:
- 10891088, a 82 yo Female, died on 2020-12-30, 125 days after her second dose of “Dementia”
The fact that a subject could die a few months after signing the forms of “Dementia” raises obvious concerns as far as “informed consent” is concerned (it’s unclear how dementia becomes the primary cause of a death).
In the 85 to 94 yo group, 1 subject died in the BNT162b2 arm.
- 10971023, a 87 yo Female, died on 2020-12-21, 98 days after her second dose of “Septic shock”
Having done the above detailed breakdown, we uncovered that 11351033 & 11311204 were often wrongly classified as deaths in the Placebo arm, while they had received a third dose (a first of BNT162b2, the active product).
Deaths during the trial vs Expected mortality
Aside from the fact that the active product miserably failed to demonstrate any benefit according to the sponsors’ data against death (21 against 17), or deaths for Covid-19 (1 in each arm), it seemed useful to compare the trial mortality with the one observed in general population, to illustrate another, more obvious issue. As pointed out by the observant Pete Lincoln9, there aren’t enough deaths documented here.
Don’t get us wrong, we aren’t wishing harm on anyone, but the trial was run on a large, theoretically quite representative population, and 38 deaths on more than 46 000 subjects seemed quite low at first sight over a 7 months period (first doses administered end July 2020, up to March 13 2021).
Said phase 2-3 trial has been conducted between 2020 & 2021, and the treatment arms have accrued different times of exposure given that unblinding has been removed for the Placebo subjects after December’s EUA (for “ethical concerns”, to protect them with the experimental product against the disease which hadn’t killed any placebo on 625 cases accrued end December).
We cross-checked the death rates observed during the trial in USA (representing most of the subjects with 35 850 of the 46 310), compared to the USA’s official ones for these age groups - available for 202010 & 202111 on the CDC’s website.
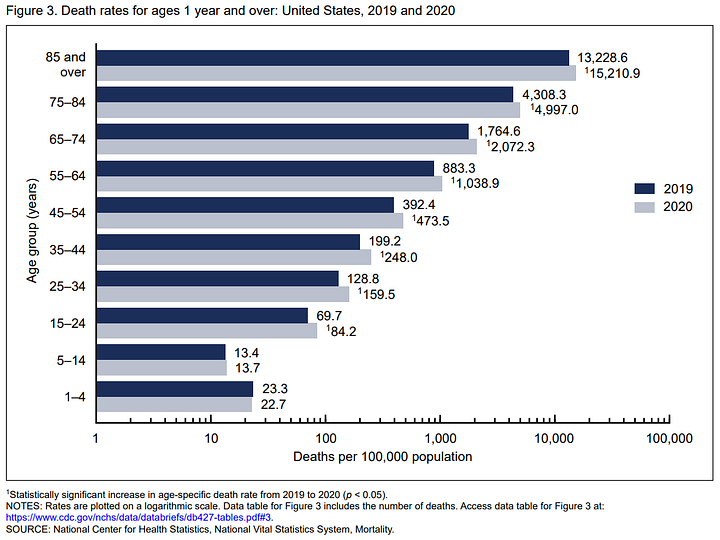
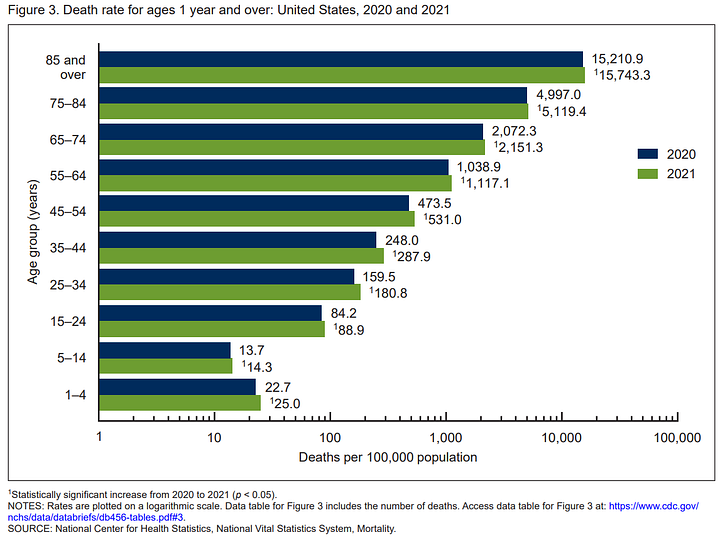
These charts, with data from 2019, 2020 & 2021, are screaming “success of the official health policy”, but they also offer normalized perspective on the death rates to expect in USA, for a population of 100.000 observed over a year.
We aren't pretending to advanced accuracy here, but to the brief illustration of an obvious point. We picked an average of the 2020 / 2021 mortality rate as reference. Deaths are seasonal (more people are dying in the cold months, October to March in most of the US, than the rest of the year12).
So, if anything, our figures on this “most cautiously observed” population should be around baseline, not far below.
We can compare these with the mortality observed during the trial to provide some (very raw) estimates of which death rates should have been observed in each group - had the tracking of “what happened to the subject” been done diligently.
For each arm, we calculated the global days of exposure accrued by the subjects (sometimes one subject was observed in different treatment arms given they could receive two placebos & two doses of the active product) to calculate a death rate / 100.000 persons / year.
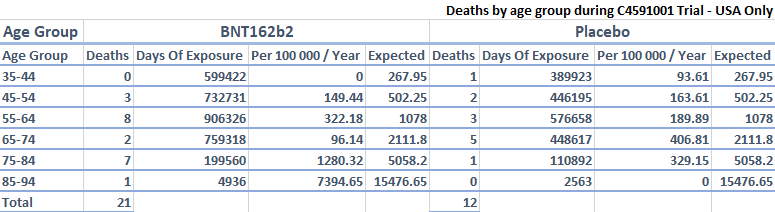
Given this chart, with every mortality rate below expected frequency, one of these two explanations is true:
- Registering in a Pfizer/BioNTech trial was magically protecting you against life hazards (aside for heart conditions)
- Tracking of the subject’s health state by the clinical trial team was beyond bad, and only a fraction of the deaths have been properly accounted for
Of course there would be some "healthy user bias", which factors as pointed out by Mathew Crawford in the general efficacy illusion13 (you may think that people choosing to participate in a clinical trial are generally more healthy than the general population).
But was it the main factor explaining the fact deaths reported were so low - particularly in the oldest age groups, in a trial were elders with Dementia were recruited? Or would it be the lack of diligence of Pfizer/BioNTech to investigate what happened to subjects lost to follow-up?
As usual, the code used to generated this analysis is available on GitHub.
💬 Join the conversation
Want to like, comment, or share this article?
Head over to our Substack page to engage with the community.
Likes, comments, and shares are synchronized here every 5 minutes.